Wednesday, January 30, 2008
Stretching Exercises
Often physicians advise their patients to do stretching exercises but due to time constraints on their schedule, they don't have the time to explain the exercises in detail. Here's a quick tutorial on stretching different muscle groups that may be helpful. This site has been a useful tool for many of my patients who are not familiar with proper stretching techniques.
Sunday, January 27, 2008
How to Treat Acne
Acne is a chronic condition, but almost all cases of acne can be treated. Appropriate management should heal current lesions, prevent new lesions and minimize scarring. It is important to remember that proper treatment of acne takes time, at least 4 to 6 weeks. Fast acting potions are false promises. It is also crucial to be consistent with therapy. Non-compliance is the most common cause of treatment failures.
The type of medication used to treat acne depends on the severity of the condition. Mild to moderate acne is treated with topical medications such as retinoids, benzoyl peroxide, salicylic acid and topical antibiotics. Topical retinoids are the foundation of treatment. They are a derivative of vitamin A and work to unclog pores and prevent whiteheads and blackheads from forming. They may cause an initial irritation of the skin in the first 2-4 weeks. This is a common reaction and can be managed by moisturizing the skin, using sunscreen and increasing the dose of the retinoid gradually. My personal choice is Adapalene (Differin) because it is non-photosensitizing (doesn't cause irritation with sun exposure) and it can be used in the mornings. Other retionids include Treinoin (Retin-A) and Tazarotene (Tazorac) which is reserved for oily skins.
In general, if the topical retinoid alone is not sufficient, then a combination of the retinoid with a topical antibiotic (newly approved Ziana Gel) or a combination of benzoyl peroxide with a topical antibiotic (Duac or Benzaclin) may be given for a broader coverage. I prefer Duac because it does not need to be refrigerated and it can be applied once a day which improves compliance.
Oral agents are used to target moderate to severe acne. These include antibiotics, isotretinoin (Accutane), birth control pills, testosterone blockers and corticosteroids. Antibiotics are the most commonly used of these options. They include tetracycline, doxycycline, minocycline, and erythromycin. Each of these has its own set of side effects. The choice of the antibiotic depends on the tolerance of side effects as well as the cost with doxycycline and tetracycline being the least expensive and minocycline being the most expensive. Antibiotics are generally given for 3-6 months and are then tapered off.
Almost all birth control pills can help reduce acne for the majority of women. They are especially useful for premenstrual flares of acne. My preferred oral contraceptive for acne is Yasmin because it helps to block the affect of androgen on the sebaceous (oil producing) hair follicles. Other pills are Demulen 1/50, Orhto-Tri Cyclen, Orhto-Cyclen, Ortho-Evra, Mircette, Brevicon, and Modicon. All of these are higher estrogen, lower androgen potency pill.
Please note that Depo-Provera, a long acting progesterone contraceptive, is often associated with acne. It needs to be avoided in patients with acne.
Severe acne with scarring may be treated with Accutane. Patients should not get pregnant during treatment with this medication because it can cause birth defects. The treatment is 20 weeks long and the major side effects are dryness of the lips. The patient should also be monitored for depression and for abnormalities in liver or cholesterol by routine blood tests.
Once the acne is controlled, there are several methods available to improve the scarred areas. These include fillers, chemical peels, dermabrasion, or laser resurfacing. These procedures may be done by a dermatologist or a plastic surgeon.
The type of medication used to treat acne depends on the severity of the condition. Mild to moderate acne is treated with topical medications such as retinoids, benzoyl peroxide, salicylic acid and topical antibiotics. Topical retinoids are the foundation of treatment. They are a derivative of vitamin A and work to unclog pores and prevent whiteheads and blackheads from forming. They may cause an initial irritation of the skin in the first 2-4 weeks. This is a common reaction and can be managed by moisturizing the skin, using sunscreen and increasing the dose of the retinoid gradually. My personal choice is Adapalene (Differin) because it is non-photosensitizing (doesn't cause irritation with sun exposure) and it can be used in the mornings. Other retionids include Treinoin (Retin-A) and Tazarotene (Tazorac) which is reserved for oily skins.
In general, if the topical retinoid alone is not sufficient, then a combination of the retinoid with a topical antibiotic (newly approved Ziana Gel) or a combination of benzoyl peroxide with a topical antibiotic (Duac or Benzaclin) may be given for a broader coverage. I prefer Duac because it does not need to be refrigerated and it can be applied once a day which improves compliance.
Oral agents are used to target moderate to severe acne. These include antibiotics, isotretinoin (Accutane), birth control pills, testosterone blockers and corticosteroids. Antibiotics are the most commonly used of these options. They include tetracycline, doxycycline, minocycline, and erythromycin. Each of these has its own set of side effects. The choice of the antibiotic depends on the tolerance of side effects as well as the cost with doxycycline and tetracycline being the least expensive and minocycline being the most expensive. Antibiotics are generally given for 3-6 months and are then tapered off.
Almost all birth control pills can help reduce acne for the majority of women. They are especially useful for premenstrual flares of acne. My preferred oral contraceptive for acne is Yasmin because it helps to block the affect of androgen on the sebaceous (oil producing) hair follicles. Other pills are Demulen 1/50, Orhto-Tri Cyclen, Orhto-Cyclen, Ortho-Evra, Mircette, Brevicon, and Modicon. All of these are higher estrogen, lower androgen potency pill.
Please note that Depo-Provera, a long acting progesterone contraceptive, is often associated with acne. It needs to be avoided in patients with acne.
Severe acne with scarring may be treated with Accutane. Patients should not get pregnant during treatment with this medication because it can cause birth defects. The treatment is 20 weeks long and the major side effects are dryness of the lips. The patient should also be monitored for depression and for abnormalities in liver or cholesterol by routine blood tests.
Once the acne is controlled, there are several methods available to improve the scarred areas. These include fillers, chemical peels, dermabrasion, or laser resurfacing. These procedures may be done by a dermatologist or a plastic surgeon.
References: please see above links.
Resources: Acne tutorial. NIH Questions and Answers about Acne. AcneNet.
Tuesday, January 22, 2008
What Causes Acne
Acne vulgaris (pimples) is a common chronic skin condition that occurs in teens and adults. It results from faulty follicular keratinization - some of the skin cells get sticky and don't exfoliate properly. This causes microcomedones. There is also sebaceous gland hyperactivity which causes an increase level of oil production by the skin. Under these conditions the skin surface bacteria, Propionibacterium acnes, proliferates more heavily which may lead to inflammatory acne. Occasionally these changes may lead to scarring.
Factors that influence acne include:
-Medications such as steroids, Lithium and other mood stabilizers as well as certain contraceptives such as depo-provera.
-Menstrual cycle
-Emotional stress which leads to higher levels of certain hormones such as cortisol and androgens
-Overproduction of androgens
-Family history
-Materials that obstruct the follicles such as helmet straps, shoulder pads, or tight headbands
-Picking
Factors that don't cause acne are:
-Chocolates, fatty food or sodas
-Poor hygiene
-Not washing the skin vigorously
You don't just grow out of this condition. There are treatments which work for acne. These will be covered in the next blog.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Factors that influence acne include:
-Medications such as steroids, Lithium and other mood stabilizers as well as certain contraceptives such as depo-provera.
-Menstrual cycle
-Emotional stress which leads to higher levels of certain hormones such as cortisol and androgens
-Overproduction of androgens
-Family history
-Materials that obstruct the follicles such as helmet straps, shoulder pads, or tight headbands
-Picking
Factors that don't cause acne are:
-Chocolates, fatty food or sodas
-Poor hygiene
-Not washing the skin vigorously
You don't just grow out of this condition. There are treatments which work for acne. These will be covered in the next blog.
Thursday, January 17, 2008
What's the Skinny on Diet Pills
 I don't advocate diet pills. There are no short cuts to long-term weight loss. However, a frequently asked question, especially during this time of the year, is what's new with diet pills.
I don't advocate diet pills. There are no short cuts to long-term weight loss. However, a frequently asked question, especially during this time of the year, is what's new with diet pills.A few years ago, the combination of phenteremine ad pondimin,( phen-fen), was quite popular. Both medications were effective appetite suppressants and they helped patients lose weight faster. However, their use was discontinued when they were associated with valvular heart disease.
Current medications which are available include orlistat (Xenical, Alli) and sibutramine (Meridia). Orlistat interferes with absorption of fats by interfering with one of the digestive enzymes in the intestines. Diarrhea, gas, and dyspepsia are the most common side effects. It results in 3 kg. (6.6 lbs.) more weight loss than placebo after 1 year.
Sibutramine suppresses appetite by working on the appetite control centers of the brain. It affects the processing of certain brain hormones such as serotonin. It was shown to result in 4.5 kg (9 lbs.) more weight loss than placebo in 1 year. The side effects include dry mouth, insomnia, and nausea.
There are several other medications which are currently under investigation but which have not yet been approved in the United States. Many of these work by by decreasing the activity of the endocannainoid system (EC). This is the same brain circuit that makes people hungry when they smoke cannabis (marijuana).
The EC system is a recently recognised physiological system that includes receptors such as the CB1 receptor and and which has been shown to play an important role in regulating body weight and in controlling energy balance. Rimonabant (also known as Zimulti, Acomplia or Slimona) has already been approved in Europe. It works by blocking the CB1 cannabinoid receptor. In one study it stopped food craving and helped overweight people lose an average of 20 pounds. It also was found to decrease craving for certain addictive substances. The side effects associated with this medication have been depression and anxiety.
{kind=link}
While these medications may have a role in short term treatment of obesity, they are not recommended for long term weight management. Each medication has its own profile of side effects. Exercise and proper nutrition remain the safest regimen although admittedly not the most immediately gratifying solution.
References: Drugs Fut 2007, 32(9): 766
Photo: courtesy of La Verne Magazine
Tuesday, January 15, 2008
Life Expectancy

Life expectancy at birth reached a record high of 78 years in 2005 for the U.S. population. The United States ranks 45 in the world in life expectancy. See here for a ranking of the other countries.
Reference: National Center for Health Statistics
{kind=link}
Sunday, January 13, 2008
Changes in Urine Color
 A patient came in today panicked because his urine had turned red. This is a frightening experience for most patients, and of course the doctor should be consulted for this condition. There are several medical conditions which may cause changes in the color of urine ranging from red to orange to brown. However, there are also some benign causes such as the types of food that have been consumed, as well as any food colorings, over-the-counter or prescription medications, or diagnostic dyes that were recently ingested.
A patient came in today panicked because his urine had turned red. This is a frightening experience for most patients, and of course the doctor should be consulted for this condition. There are several medical conditions which may cause changes in the color of urine ranging from red to orange to brown. However, there are also some benign causes such as the types of food that have been consumed, as well as any food colorings, over-the-counter or prescription medications, or diagnostic dyes that were recently ingested.{kind=link}
Althought this is probably more detail than you would ever want to know about your urine, here is a very complete review by Dr. Martha Terris of the possible causes of different urine colors.
The normal color of urine ranges from light yellow to dark amber, depending on the concentration of solutes in the urine. The more dehydrated that the body is the darker yellow the color of the urine may look. Urochrome is the name of the pigment that gives urine its characteristic yellow color. Other urinary complaints may accompany changes in urine color. Such symptoms include urinary urgency (having to hurry to get to the bathroom), frequent urination, burning pain with urination (indicative of infection), or colicky pains (suggesting kidney stones).
Pink or red urine should prompt an immediate visit to your doctor. The first test is a dipstick for blood. A positive dipstick for blood implies the presence of red cells, free hemoglobin (from broken down red blood cells), or myoglobin (from broken down muscle cells).
{kind=link}
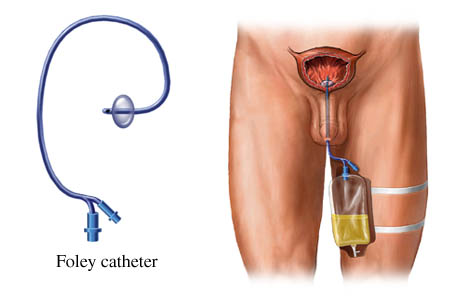
Red blood cells in the urine may be from kidney loss (termed "glomerular" blood cells) in patients with renal disease. Red cells in the urine of these individuals will usually be misshapen and accompanied by protein in the urine. Normal appearing red blood cells (termed "epithelial" red blood cells to identify them as cells coming from the lining of the urinary tract instead of the kidney) may be present during a urinary tract infection, urinary stone, or urinary malignancy. Red blood cells are common in the urine after urologic procedures and occasionally following catheter placement. Complete urine testing (called "urinalysis") for the presence of bacteria and white blood cells, urine culture, cystoscopy, CT scan, and/or other imaging studies may be necessary to clarify the source of the blood.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
If the urine is red and acid but does not contain hemoglobin, myoglobin, or red blood cells, suspect an indicator dye such as phenolphthalein (the laxative in ExLax) in which case the red should disappear when the urine is alkalinized with a few drops of potassium hydroxide. Blackberries and beets can turn acid urine red due to the presence of anthrocyanin, while rhubarb, anthraquinone laxatives, and some diagnostic dyes will redden urine only when it is alkaline. The anesthetic, propofol, has been reported to cause pink coloration of the urine, particularly in alcoholics. Other medications that can cause red urine are the phenytoin, phenothiazines, e.g., Compazine. Red urine can also be caused by chronic lead and mercury poisoning.
Orange urine may be produced by phenazopyridine (Pyridium) or ethoxazene (Serenium), both of which are used as urinary tract anesthetics to diminish urinary discomfort. Rifampin, phenacetin, sulfasalazine, Vitamin C, riboflavin, and carrots will also turn urine dark yellow to orange. An opaque orange-pink urine color can result from abundant uric acid crystals which can be seen in acidic urine of patients who have undergone intestinal by-pass surgery or are receiving chemotherapy for malignancy.
Blue or green urine may be caused by a blue dye such as methylene blue, a component in several medications (Trac Tabs, Urised, Uroblue) used to reduce symptoms of bladder inflammation or irritation. Administration of the dye, indigo carmine, turns the urine green and can last for several days if renal function is poor. While more often reported to cause pink urine, the anesthetic, propofol, has also been reported to cause green coloration of the urine. Amitriptyline, indomethacin, resorcinol, triamterine, cimetidine, phenergan, and several multivitamins also lend a blue-green tint to the urine. An inherited form of high calcium (called "familial hypercalcemia") can result in blue urine, which has lent this disease the nickname "blue diaper syndrome". Another metabolic disorder, indicanuria, can cause blue urine due to tryptophan indole metabolites. A blue pigment may also be produced by infection with the bacteria Pseudomonas . Dark green pigmentation, especially if associated with air (known as "pneumaturia"), urinary tract infection, and/or solid particles in the urine, can be caused by bile when there is a fistula between the urinary tract and the intestines.
Brown or black urine (not due to myoglobin or bilirubin) may be caused by excessive L-dopa or melanin excretion as well as copper or phenol poisoning. Ingestion of large amounts of rhubarb, fava beans, or aloe can cause dark brownish black urine. Metabolites of the antihypertensive medication methyldopa (Aldomet) may turn black on contact with bleach (which is often present in toilet bowls) . Other medications causing brown or brown-black urine are chloraquine and primaquine, furazolidone, metronidazole, nitrofurantoin, cascara/senna laxatives, methocarbamol, and sorbitol. Contamination with povidone-iodine (Betadine) solution or douche can turn urine brown. Melanin and melanogen, found in the urine of patients with melanoma, will darken standing urine from the air-exposed surface downward. Alcaptonia, a rare hereditary disease, will turn the urine dark after being exposed to the air over a period of time due to the presence of homogentisic acid. Urinary hydroxyphenylpyruvic acid excretion due the metabolic disorder tyrosinosis will also cause urine to be brown-black in color. In porphyria cutanea tarda, the urine will appear reddish brown in natural light but fluoresces pink under ultraviolet light.
White or cloudy urine is most commonly a result of phosphaturia. This is a benign condition in which excess phosphate crystals form in urine. Adding a drop of acetic acid to the urine sample will result in immediate clearing of the urine. Phosphaturia is usually intermittent, occurring following a meal or after ingesting a large quantity of milk. White urine is sometimes due to pyuria (abundant white blood cells) in association with an infection of the urinary tract. White cloudy urine can rarely be due to chyluria (lymph fluid), resulting from a communication between the lymphatic system and the urinary tract.
Please contact your physician with any concerns that you may have.
Reference: Dr. Martha Terris.
Photo: courtesy of News Target
Thursday, January 10, 2008
Asthma Control Test
If you have asthma, take this test and share the results with your doctor.
The Asthma Control Test (ACT) is designed to give you an idea of how well your asthma has been controlled over the last 4 weeks. It can also help your doctor determine how well the treatment plan is working for you.
The test is for ages 12 and older. It consists of 5 simple questions which are scored individually. The maximum score is 25. If your score is less than 20, it means that your asthma is not well controlled. The test can be taken at any time. and since asthma symptoms may vary it may be worthwhile to use this test at regular intervals or if you sense a change in your condition.
The National Heart, Lung, and Blood Institute recently recognized ACT as a validated instrument for the assessment and monitoring of asthma in its Guidelines for the Diagnosis and Management of Asthma.
The Asthma Control Test (ACT) is designed to give you an idea of how well your asthma has been controlled over the last 4 weeks. It can also help your doctor determine how well the treatment plan is working for you.
The test is for ages 12 and older. It consists of 5 simple questions which are scored individually. The maximum score is 25. If your score is less than 20, it means that your asthma is not well controlled. The test can be taken at any time. and since asthma symptoms may vary it may be worthwhile to use this test at regular intervals or if you sense a change in your condition.
The National Heart, Lung, and Blood Institute recently recognized ACT as a validated instrument for the assessment and monitoring of asthma in its Guidelines for the Diagnosis and Management of Asthma.
Sunday, January 06, 2008
Fish Oils May Prevent Alzheimer's Disease
 A recent study from the University of California Los Angeles Departments of Medicine and Neurology concludes that fish oils may help prevent Alzheimer's disease. The researchers found that omega-3 fatty acid docosahexaenoic acid (DHA), which is found in fish oil, raises the production of LR11, a protein which destroys the plaques in the brain which have been associated with Alzheimer's disease.
A recent study from the University of California Los Angeles Departments of Medicine and Neurology concludes that fish oils may help prevent Alzheimer's disease. The researchers found that omega-3 fatty acid docosahexaenoic acid (DHA), which is found in fish oil, raises the production of LR11, a protein which destroys the plaques in the brain which have been associated with Alzheimer's disease.These plaques which are toxic to the brain cells are deposits of a protein called beta-amyloid.
{kind=link}
Patients with late-onset Alzheimer's disease tend to have a high number of these plaques and very low levels of LR11. Both genetic and environmental factors may contribute to this process.
The scientists administered the fatty acid by diet to mice and also directly to cultured human neuronal cells to evaluate its effects. They found that even low doses of DHA increased the level of LR11 in the brain cells. "Consequently, elevated levels of DHA, which in turn lead to an abundance of LR11 appear to protect against Alzheimer's disease, while low LR11 levels have the opposite effect as they allow the formation of the amyloid plaques."
DHA is considered an "essential" fatty acid because it can only be obtained through diet. Our bodies cannot produce it from any other source. It is also the most abundant essential fatty acid in the brain and has been known to be important for healthy brain development in the fetus.
{kind=link}
Other benefits of omega-3 fatty acids include lowering cholesterol and triglyceride levels, cardiovascular protection, and anti-inflammatory and anti-blood clotting actions. They have also been reported to help reduce the risks and symptoms for other disorders such as rheumatoid arthritis, asthma, psoriasis, eczema, inflammatory bowel disease, ulcerative colitis, and depression.
{kind=link}
As a result of these findings, the National Institute of Health is currently carrying out a large-scale clinical trial with DHA in patients with established Alzheimer's disease. Further studies are needed to confirm these findings and to establish a dose that may be helpful in the prevention of the disease.
References: please see above links.
Photo: courtesy of Pharma Gazette.
Tuesday, January 01, 2008
Hold On to Your Resolutions
Here's a quick tip to help you to stick to your resolutions. Whether you have resolved to lose weight, to exercise, or to quit smoking, 90 percent of people give up on these resolutions in 2 to 3 weeks. However, it takes at least 30 days to begin to change a bad habit into a positive routine. So what ever goal you are setting, commit to it for the next 30 days. Instead of saying you want to exercise more this year, you may want to say that you will exercise more for the next 30 days. Hopefully after that period of time, the next 30 days will be easier, and so on and so on.
Subscribe to:
Posts (Atom)